




I consider myself a “vaccine-injured” fellow these days, like many others who are “quarantined” on social media for fear of “misinformation”, even from that of scientific journals, and it’s been almost two years since I first had symptoms. I think the symptoms were provoked by a legitimate sinus infection one month after “vaccination” with Moderna, but it exploded to be an “acute” respiratory inflammation situation, where an MRI led doctors to think for a moment that I had a cyst in my sinus cavity, but really, my sinuses were swollen shut and/or filled with fluid. This response was similar for my lungs, throat, and ears, where I could hardly hear anything because it was all muffled. These symptoms still return when I do such terrible things as consuming salt.
Similar inflammation happened with my breathing capacity, and due to swollen red feet and veins, it was eventually concluded that there was dysautonomia and then later POTS (although not myocarditis as yet). I had all kinds of other symptoms that led to inability to do anything, extreme diet restrictions, no exercise, constant dizziness, brain fog, and etc. Just going purely on how it felt, either I was asymptomatic with Long COVID for a long time, only to have it awakened in me later, or the vaccine caused an immune reaction the moment the immune system was compromised. The latter is making more and more sense to me as time goes on.
To add insult to injury, I had been given a booster one month later, with symptoms I’d hoped would improve still in tow, and they gave me Pfizer instead of the Moderna I had been “vaccinated with” prior. They said the mix up would give “added immunity”. The receptionist refused to write on my vaccine card that I had been given Pfizer instead of Moderna, they were just simply out of Moderna. Some sites say that mixing and matching different products is fine, but I would venture to disagree. That very evening, I just coincidentally began nine months where every day was a blackout, struggling to avoid seizures, with what they now call “air hunger”. The pulmonologist told me to drink more water, and go for a walk. Naturally, I came to ask a lot of questions.
What eventually got me out of a state of struggling for air was what doctors specifically told me not to try: A nebulizer with purified water and a couple drops of food grade 3% Hydrogen Peroxide (I am not a doctor, not giving medical advice, and definitely not saying you should huff straight Hydrogen Peroxide for an hour at a time, like doctors seemed to think I would). There was also this crazy frequency generator that my friend (eternal thanks to Leslie) ran for me every day. There were some days where I was seeing black spots and strobe effects, and this woo woo thing, with some little box that contained my most recent fingernail clippings, surprisingly worked on helping me breathe. I could tell when she turned it off at night, because it became much more difficult to breathe.
I am still not out of the woods. The last time I tried more than twenty push-ups, or squats, I felt like my bones were rotting and on fire. My joints and my muscles felt like there were needles everywhere poking me from the inside. I can’t eat much without consequences. It’s mostly soup and salad, unless I am ready to feel like I have been hit by a truck in the morning, and the dizziness didn’t help for the first year especially. I have found gluten-free this and keto that can help, and meat can be tricky, among other things. I have spent hundreds of dollars on vitamin supplements and weird remedies. I left one medical center to go to another that gave me more meds that caused wild side effects, so I have rejected them all, especially when they gladly give eachother Covid without masks on.
I have been to the emergency room with severe chest pains, and they gave me Tylenol, and after a few scans, said there was nothing wrong with me. In my experience, and in my opinion, I really thought I was going to die every day for a while, and I didn’t know why I was still alive. It made no sense to me. My resting heart rate was up to 212 at one point, I always felt that I was going to faint, chronic fatigue had me sleeping 20 hours a day for a while, and at other times it was totally stable. So anyway, when people say there isn’t a “causal link” between the vaccine and adverse reactions, I beg to differ. I had an adverse event right after getting the booster, and the only reason I didn’t go to the hospital was because I know ventilators aren’t great for stopping the spread of Covid.
I think that The FDA, The CDC, and all who support their flagrant lies, should be ashamed of themselves. The vaccine has harmed a great many people who had not had Covid prior, and even some that did. There is no reason to call what they did to the human race “informed consent”, as the vaccine does not technically prevent transmission, and it has been found to cause more immune problems later on, to say the absolute least about all of the long term problems that are starting to arise from these vaccines.
How can something be “safe and effective” after such a short period of development?
Janssen and AstraZeneca vaccines were recalled rather quickly, while Pfizer and Moderna vaccines are still pushing along. I can only gather that there was an unacceptable amount of adverse events, or that they happened too quickly, before the control groups stopped testing. Or maybe their profit margin was too low to handle the amount of lawsuits that they would be getting outside of the states, where liability is still allowed by law. It seems that, after 30 days, any adverse events can be blamed on something else, not that any vaccine manufacturers have liability or incentive to produce a quality product. The authorities can deny any “causal” link to injuries, and a special (“black hole”) system that operates independently of the judicial branch of government, and “expedites” vaccine injury claims with impunity in the United States.
Yes, I have gone down that rabbit-hole. I now question the advocacy of vaccines throughout their entire history, when compared to improvements in sanitation, hygiene, and diet. I don’t know why they use ethyl-mercury for vaccines, but I think they should call it something else, like “ethyl-electrolytes” or something. I don’t think they know enough about the blood-brain barrier to say definitively that aluminum is just fine to inject into a person, and I won’t likely be convinced on the subject while psychiatry is still just a series of gross generalizations and guess work.
And anyway, I’m no longer convinced that the testing, since there is no longer liability, was ever stringent enough. I think more people should know that aborted babies were used in the culturing of vaccines, because I know plenty of people who would not go for it, I’m not talking about evangelical Christians either. The distributed model for vaccines was much different than what was approved by the FDA. Pfizer has a history of distribution errors with vaccines, up to and including glass particles in the doses, with no apparent consequences to date, until recently.
I personally am an advocate of quarantine and masks rather than taking an experimental chemical that would have been recalled by any stretch of the imagination, if the same liability as baby formula were applied. The appeal to authority fallacy is in full effect, in place of common sense and logic. I took the vaccine because I wanted to be able to leave the country, despite having a bad feeling, yet I never did leave the country, unfortunately. It shouldn’t really be that much of an argument.
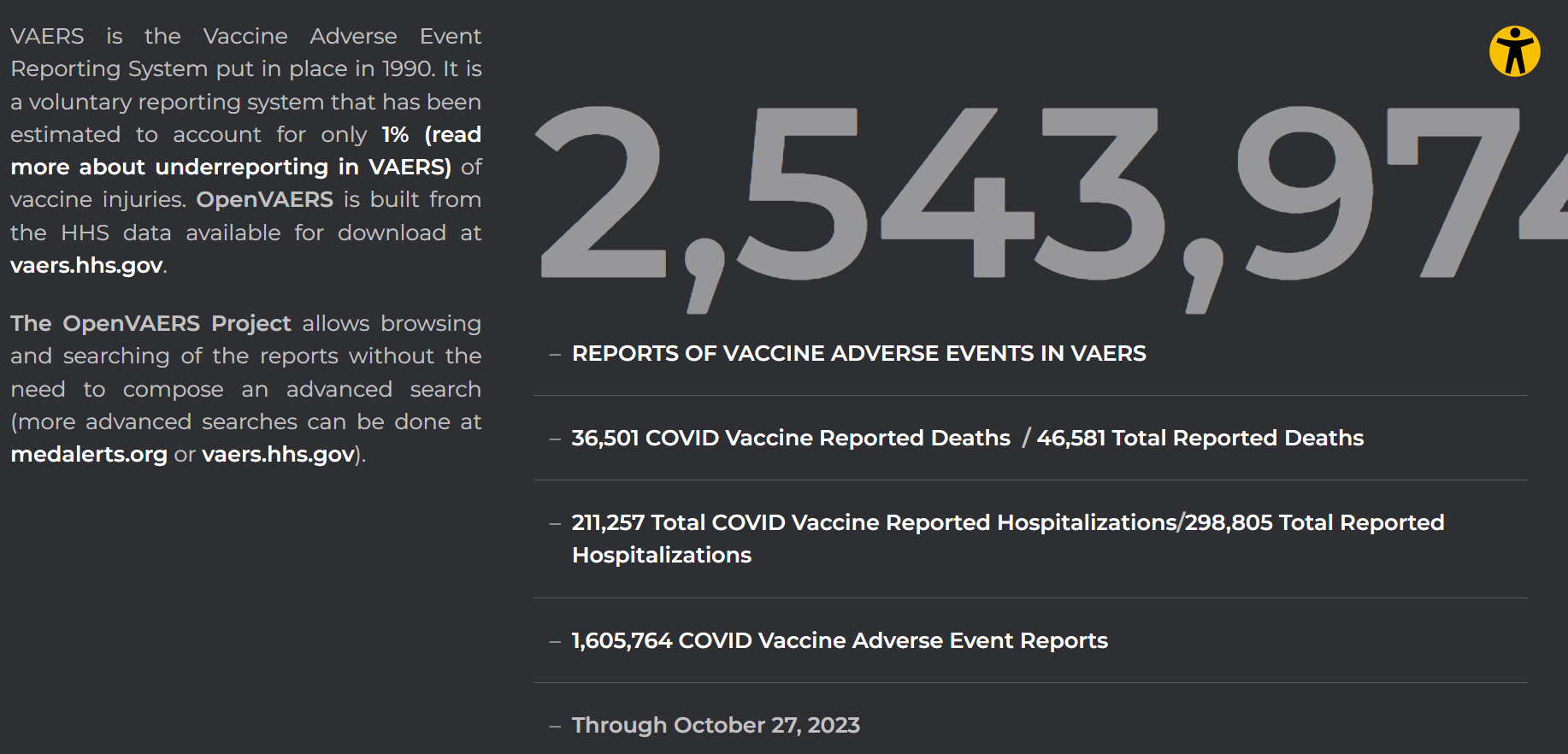
The VAERS database states clearly that it estimates only 1% of adverse events from vaccines are reported, and there are over 36,500 in the United States alone at this moment. So if we estimate based on their characters, we can say that probably about the size of the entire population of Puerto Rico, with some to spare, has had an adverse event from the Covid vaccines alone. My doctors refused to report my case to the VAERS database, and I was told by VAERS to send them all of my medical history from every medical center, which is still in progress… No wonder their numbers are so low. If they have scaled back reporting like they have done with Covid cases, it should be a concern, but instead, there is just the mantra: “safe and effective”. It’s easy to say the pandemic went away, if you stop reporting it.
Here I will collect various links that have been rapidly accumulating, so that people can see, for example, independent studies that are happening outside of the United States, where the FDA, the CDC, and media in general have shut down any presentation of evidence to the contrary of their particular narrative, which is, “vaccines are 100% safe and effective” and “trust the science”, where supporting evidence in favor of vaccines is most often either not provided, or funded by pharmaceutical companies. And no, I’m not going to throw the baby out with the bathwater like I think RFK, Jr. did, because I don’t know enough about HIV, much less its treatment, to say that it was a medical holocaust of sorts (his words, not mine), but I will say that people who would dismiss me as a conspiracy theorist, in a way, are looking a lot more like holocaust deniers, with all due respect.
1,000 Peer-reviewed Articles On Vaccine Injuries.
Not Nobel: Not effective, not safe | "Professor Richard Sandberg said 13 billion people had got the virus before correcting himself and saying the vaccine. It was not so much a Freudian slip as a statement of fact since virtually everyone who has got the vaccine has gotten the virus."
“…The scientist who invented mRNA vaccine technology (and holds the patents, with others) is Dr. Robert Malone. He was asked this week if he should also have been given the Nobel. His reply? ‘Probably not because the technology has not been proven safe’”.
IgG 4 related disease (IgG4-RD) is a systemic fibroinflammatory disease characterized by dense infiltration of IgG4-positive plasma cells in the affected tissue(s) with or without elevated plasma levels of IgG4.1 The inflammatory infiltration along with a characteristic storiform fibrosis can lead to the development of chronic damage and/or tumefactive lesions1 that may affect any organ.
Autoimmune inflammatory reactions triggered by the COVID-19 genetic vaccines in terminally differentiated tissues
The spike protein can independently cause damage, regardless of interaction with ACE2 receptors. The only difference between the spike protein in the virus vs the vaccine is that the one in the vaccine has a tiny tweak that limits its interaction with ACE2: it does not shape to "post fusion" shape. This could be why vaccine-injured have similar symptoms to Covid.
Nearly a quarter of Americans believe someone they know died from COVID-19 vaccine side effects, and even more say they might be willing to become plaintiffs in a class-action lawsuit against vaccine makers.
An interview with Dr. Phillip Buckhaults about DNA contamination in covid vaccines.
Australia: The discovery of excessive levels of DNA contamination in the mRNA COVID shots has raised questions about how it got there, and what it means for people who may have been injected with contaminated products. Scientists have some answers, and a lot of questions…
‘Spikeopathy’: COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA… Seven Australian Authors Publish Comprehensive Peer-Reviewed Paper Concluding Genetic Vaccines Must be Pulled
Fully-Vaxxed New Zealand Suffers 3000% Spike in Excess Deaths (Slay News); Official data shows that 95.8% of the eligible New Zealand population aged 12 & over have received one dose of COVID vaccine
Now a study funded by the Dutch government, currently available as a preprint, provides further evidence that the mRNA COVID-19 jabs are increasing IgG4 antibodies. The researchers state: “Repeated mRNA vaccination against SARS-CoV-2 has been shown to induce class switching to IgG4, a non-inflammatory human antibody subclass linked to tolerance.
Proof Regarding the Clinical Trials Relied Upon by the FDA to License the Childhood Vaccines on the CDC Childhood Vaccine Schedule
Vaccinated children were significantly more likely than the unvaccinated to have been diagnosed with the following: allergic rhinitis (10.4% vs. 0.4%, p <0.001; OR 30.1, 95% CI: 4.1, 219.3), other allergies (22.2% vs. 6.9%, p <0.001; OR 3.9, 95% CI: 2.3, 6.6), eczema/ atopic dermatitis (9.5% vs. 3.6%, p = 0.035; OR 2.9, 95% CI: 1.4, 6.1), a learning disability (5.7% vs. 1.2%, p = 0.003; OR 5.2, 95% CI: 1.6, 17.4), ADHD (4.7% vs. 1.0%, p = 0.013; OR 4.2, 95% CI: 1.2, 14.5), ASD (4.7% vs. 1.0%, p = 0.013; OR 4.2, 95% CI: 1.2, 14.5), any neurodevelopmental disorder (i.e., learning disability, ADHD or ASD) (10.5% vs. 3.1%, p <0.001; OR 3.7, 95% CI: 1.7, 7.9) and any chronic illness (44.0% vs. 25.0%, p <0.001; OR 2.4, 95% CI: 1.7, 3.3).
When the Covid-19 vaccines rolled out, public health officials took great pains to downplay how the vaccines spread from the injection site. Articles with language like this were common: “Most of the mRNA vaccine stayed in the injection site muscle—where you get the shot.”
We now know the truth. The lipid nanoparticles, or LNPs, travel widely throughout the body. These LNPs carry the Frankenstein mRNA that causes the cells to produce spike proteins.
COVID-19 vaccine-associated mortality in the Southern Hemisphere:
Seventeen equatorial and Southern-Hemisphere countries were studied (Argentina, Australia, Bolivia, Brazil, Chile, Colombia, Ecuador, Malaysia, New Zealand, Paraguay, Peru, Philippines, Singapore, South Africa, Suriname, Thailand, Uruguay), which comprise 9.10 % of worldwide population, 10.3 % of worldwide COVID-19 injections (vaccination rate of 1.91 injections per person, all ages), virtually every COVID-19 vaccine type and manufacturer, and span 4 continents.
New British government data showing mRNA vaccinated dying 52% more than unvaccinated - aka 1.5x accelerated death rate
Batch-dependent safety of the BNT162b2 mRNA COVID- 19 vaccine (European Journal of Clinical Investigation)
100% of Covid-19 Vaccine Deaths were caused by just 5% of the batches produced according to official Government data
FDA Sued Over Hiding Records From Moderna COVID-19 Vaccine Approval
Elaborate breakdown of how widespread vaccination data is misrepresented in scientific papers.
Leaked documents show that some early commercial batches of Pfizer-BioNTech’s covid-19 vaccine had lower than expected levels of intact mRNA, prompting wider questions about how to assess this novel vaccine platform
UK Scientist Reveals Data Analysis: Some Batches Are 50 Times Worse Than Others.
The specter of particulates has forced another recall—this time on Moderna’s massively successful COVID-19 vaccine Spikevax—and the latest pull isn’t contract manufacturer Rovi’s first brush with contamination, either.
Japan finds another Moderna vial suspected to contain foreign substance
Vietnam province suspends Pfizer vaccine batch after 120 children get hospitalized
The BioNTech/Pfizer and Oxford/AstraZeneca coronavirus vaccines are associated with seven rare neurological complications, according to the most comprehensive study of the side effects from the two jabs.
U.S. Federal Court prove Pfizer, the FDA & Fact Checkers lied when they said Toxic Graphene Oxide was not inside the Covid-19 Vaccines
DNA should not be more than 0.033 per cent of the total nucleic acids in the dose. But McKernan’s analysis demonstrated DNA contamination of up to 35 percent in the bivalent injection samples. This is up to 1,000 times higher than deemed to be ‘acceptable’ by the regulating authorities.
Hepatitis C Virus Reactivation Following COVID-19 Vaccination
Bad Pfizer Vaccine Batches Account for 4.2% of doses but 71% of Serious Adverse Events
How did MRNA technology go from having safety issues in 2017 to being “completely safe and effective” in 2020?
Cardiovascular, neurological, and pulmonary events following vaccination with the BNT162b2, ChAdOx1 nCoV-19, and Ad26.COV2.S vaccines: An analysis of European data
DNA fragments detected in monovalent and bivalent Pfizer/BioNTech and Moderna modRNA COVID-19 vaccines from Ontario, Canada: Exploratory dose response relationship with serious adverse events.
FDA Finds Safety Signal for COVID-19 Vaccination Among Toddlers
Would Australians have consented if they knew the potential risks?
More evidence COVID jabs damage heart cells
Pfizer now admits the vaccine causes myocarditis.

Piercing the Veil of Silence over Excess Deaths | MP Andrew Bridgen speaks out | "Around the world, there has been a deafening silence over excess deaths from governments and the mainstream media, who not so long ago were quite fixated on the daily death toll for Covid."
SV40: On contamination, monkey viruses and their parts
“These mRNA shots differ completely from all other previously available “vaccine” products, not only because of their mRNA component, but also because of LNP components. LNPs are the engineered additive used to attach and deliver mRNA genetic coding for Covid-19 spike into the cells of a patient for the purpose of making mRNA stable and permit cellular absorption and transcription. Without LNPs, any RNA product would rapidly degrade. Having worked with RNA in the laboratory, I can also personally attest to RNA’s extreme fragility. “
A secondary analysis of the phase 3 RCTs where they found 16% more serious adverse events in the vaccine group.
V-Safe data showed that 7% of the vaccinated required hospitalization
2021 Australian government data which shows 20x more adverse events per 100k vaccinated compared to other vaccines.
The attorney Thomas Renz has discovered that the Department of Defense is altering data to hide the number of service members who have been injured by the experimental and deadly COVID vaccines.
Risk of immunodeficiency virus infection may increase with vaccine-induced immune response
More indication that the spike protein may be independently causing heart damage
What are the real risks of myocarditis after Covid infection and after Covid vaccine?
It has been shown now that the vaccinated equally catch and spread the virus.
Half of Vaccinated People Never Stop Producing Spike Protein, Study Found
mRNA & Breastfeeding: COVID-19 vaccine mRNA found in Breast Milk
Chinese Load Cow's Milk with mRNA Exosomes--Successfully Immunize Mice
Michigan judge denies drug manufacturer's immunity in case of contaminated COVID-19 medication
SARS-CoV-2 vaccination was associated with higher risk of myocarditis death, not only in young adults but also in all age groups including the elderly. Considering healthy vaccine effect, the risk may be 4 times or higher than the apparent risk of myocarditis death. Underreporting should also be considered. Based on this study, risk of myocarditis following SARS-CoV-2 vaccination may be more serious than that reported previously.
Science and our health authorities told us that “myocarditis is much more frequent from Covid than from vaccination”. The thing is, it was not true.
A new study from Scandinavian countries is out:
The authors worked for health departments of the four Nordic countries. They were tasked with looking at their entire populations (and their computerized records), seeking out instances of myocarditis. They had vaccination records for all people as well.
The Real Outcomes are Likely Worse
Several known facts make the picture even worse than the article presents. Numerous myocarditis cases caused by vaccines result in sudden deaths and not hospitalizations. The University of Heidelberg study shows that 20% of sudden post-vaccination deaths that they autopsied are due to myocarditis.
Those sudden deaths are NOT included in the numbers presented by the Scandinavian scientists.
Also, the study notes that some people had vaccines, Covid, and myocarditis in one 30-day interval. For those people, the cases were added to the vaccine or Covid counts based on what happened later (vaccine or Covid).
17 percent of teenagers had heart symptoms after their second Pfizer mRNA jab, a new peer-reviewed paper shows
A compendium to add to the compendium:
Revisiting the claim that “myocarditis is more common after covid than after the vaccine”
What is the evidence for these assertions?
This is a statement often made in response to concerns raised about the incidence of myocarditis after the mRNA injections. The source of this has been a number of deeply flawed papers, the most recent of which was a “systematic review and meta-analysis” published in Frontiers. This claimed a 7-fold difference between myocarditis risk after infection vs mRNA vaccine.
The claim – which contradicts several other studies, including this massive Nordic study covering 23m subjects published in JAMA – has been expertly analysed in this Twitter thread by @sborg40, an account with a profile of “Retired Infectious Disease Physician”.) – has been expertly analysed in this Twitter thread by @sborg40, an account with a profile of “Retired Infectious Disease Physician”.
A meta-analysis is a method whereby the data from many different studies are combined into one analysis. The idea is that by increasing the number of subjects covered, the results are more reliable and representative and hence statistically more powerful. However, the outcome of such an analysis is entirely dependent on (amongst other things) the studies which are used, and in fact the main criticisms of the Frontiers paper relate to the specific studies selected.
For the paper, the authors found 763 potentially relevant studies but whittled these down to only 22 (3%) for inclusion in the analysis. The Twitter thread lists the shortcomings identified which we do not intend repeating here, but in brief some of the issues @sboprg40 found with the studies which were considered for the analysis were:
3 of the 10 studies of myocarditis after covid had evidence of bias compared to none of the 12 studies after vaccination
One study was conducted by the CDC without peer review, this study looking only at the hospitalized and failing to examine all those infected
Some studies were conducted in the elderly, in ITU patients and severe covid with accompanying non-specific cardiac damage
Myocarditis diagnoses were accepted by authors without specific diagnostic criteria, in one study diagnoses were merely “probable”
Covid diagnoses were not consistent and reliable
Overall therefore, this meta-analysis contributes little to answering the core question of interest: does mRNA vaccination in the healthy young population increase the risk of myocarditis at all, and if it does how does it compare to the risk from a covid infection?
One of the most comprehensive studies looking at the risk of myocarditis after covid infection was this study out of Israel (which has an advanced and comprehensive electronic medical records system), covering a large population of nearly 200k subjects.
The authors “did not observe an increased incidence of either pericarditis or myocarditis in adult patients recovering from COVID-19 infection”.
This is, of course, entirely consistent with what is the strongest (and also simplest) evidence against the core claim, which is that numerically an increase in myocarditis cases simply wasn’t a feature of 2020, but rather this started in 2021.
Figure 1: Incidence of myocarditis across 40 hospitals in USA
{kind=link}
...
Heath Advisory and Recovery Team: Myocarditis began with vaccine rollout
More data to back up myocarditis concerns
There are two key points regarding post vaccination heart issues that HART have been raising concerns about since early 2021.
Myocarditis is attributable to injection not infection
What has been diagnosed may represent wider harm that is yet to be properly measured
...
Many people have claimed that it is the virus that is the underlying cause for myocarditis rather than the vaccinations. There are several ways to check this hypothesis. The obvious one is to compare the rate of myocarditis after infection in:
a) uninjected uninfected
b) uninjected infected
c) injected uninfected
d) injected infected
Although there have been several epidemiological analyses of myocarditis, that simple comparison is never made. Where uninjected people are looked at specifically, there is no evidence of an increase in incidence. HART has previously summarised the data after infection in the injected compared to the uninjected.
An alternative approach is to look at how common myocarditis is over time. Did the incidence increase with the arrival of covid in 2020 or the arrival of injections in 2021?
There are now several sources of data to answer that question and they all concur.
...
All three studies demonstrate a far higher rate of subclinical harm from injection than the rate measured when only looking at hospitalizations that result in a myocarditis or pericarditis diagnosis.
...
Heath Advisory and Recovery Team: Myocarditis concerns grow
HART has been trying to raise awareness for over two years.
A new study performed on adolescents in Hong Kong who suffered myocarditis after mRNA injection in Circulation appears to be generating quite a lot of discussion over how common it is, and what the long-term outcomes are for those unfortunate enough to suffer from this side effect.
Broadly speaking, the more we learn, the worse it looks.
...
Since then, we have also written about further worrying data emerging, especially regarding subclinical cases which are only found by measuring troponin levels systematically. This is logistically simple to perform, so it is criminal that it wasn’t done as soon as the signal of potential harm emerged.
...
A new scientific study by Nakahara et al. tested COVID-vaccinated people to see if they have “silent” changes in heart muscle function that standard radiology tests could detect. The study shows very unsettling results.
...
Scientists measured myocardial 18Fluorine-fluorodeoxyglucose (18F-FDG) uptake. F-FDG has molecular similarity to glucose. However, 18F-FDG does not metabolize like glucose. Therefore, PET scans could detect it, and its presence shows the heart muscle’s abnormally high demand for glucose, indicative of abnormal cardiac function. ...
Conclusions: Focal myocardial 18F-FDG uptake seen on oncologic PET/CT indicates a significantly increased risk for multiple myocardial abnormalities.
Indeed, this is what the Nakahara study finds:
Results
The study included 303 nonvaccinated patients (mean age, 52.9 years; 157 females) and 700 vaccinated patients (mean age, 56.8 years; 344 females). Vaccinated patients had overall higher myocardial FDG uptake compared to nonvaccinated patients (median SUVmax, 4.8 vs median SUVmax, 3.3 ; P < .0001). Myocardial SUVmax was higher in vaccinated patients regardless of sex (median range, 4.7-4.9 ) or patient age (median range, 4.7-5.6) compared to corresponding nonvaccinated groups (sex median range, 3.2-3.9; age median range, 3.3-3.3; P range, <.001-.015). Furthermore, increased myocardial FDG uptake was observed in patients imaged 1-30, 31-60, 61-120, and 121-180 days after their second vaccination (median SUVmax range, 4.6-5.1) and increased ipsilateral axillary uptake was observed in patients imaged 1-30, 31-60, 61-120 days after their 2nd vaccination (median SUVmax range, 1.5-2.0) compared to the nonvaccinated patients (P range, <.001-<.001).
This was not supposed to happen! The COVID vaccine is not supposed to affect the heart in any way. It was promised to “stay in the arm.”
The explosive findings of the study are discussed in the editorial that the editor of the magazine, Dr. Bluemke, felt obliged to publish.
Dr. Bluemke’s editorial is somewhat apologetic, and he gives faint praise for COVID vaccines.
The development of messenger RNA (mRNA) COVID-19 vaccines is a remarkable biotech story. While traditional vaccines took 5-10 years to develop, the COVID-19 vaccines took less than a year. By comparison, the fastest conventional vaccine previously developed was the mumps vaccine, on a timescale of 4 years.
Dr. Bluemke also does not mince words. He explains that the findings are not due to chance:
The main results: asymptomatic patients vaccinated for COVID-19 before PET had about 40% greater radiotracer activity in the myocardium than unvaccinated individuals. The P value was low, less than .0001. This translates to only 1 time out of 10 000 that these results would occur by chance.
The editorial states that there is no rational way to ignore and explain away the negative findings of myocardial inflammation by Takahara et al.:
Vaccine manufacturers are aware of the adverse effects of mRNA vaccines. These adverse effects lead to vaccine hesitancy. The study results by Nakahara et al suggest that mild asymptomatic myocardial inflammation could be more common than we ever expected. This in turn would support a hypothesis of more severe systemic inflammation related to mRNA vaccination in some patients who present with symptoma-c myocarditis.
...
Excerpt:
One of the authors of the study is from the US Food and Drug Administration.
From the article:
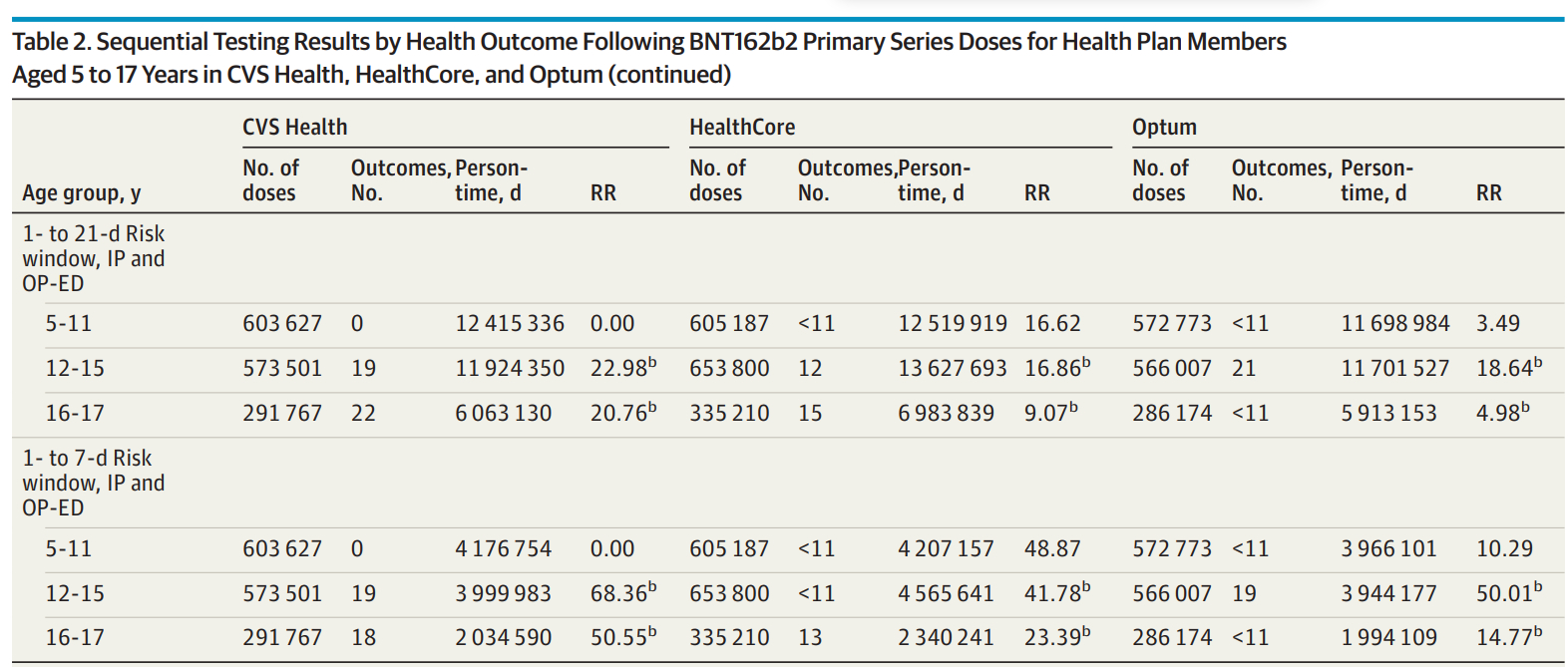
Question Does active monitoring detect potentially elevated risk of health outcomes after BNT162b2 COVID-19 vaccination in the US pediatric population aged 5 to 17 years?
Findings In this cohort study of more than 3 million children (aged 5-17 years) who received BNT162b2 COVID-19 vaccination through mid-2022 using data from 3 US commercial claims databases, only myocarditis or pericarditis met the statistical threshold for a signal after BNT162b2 COVID-19 vaccination via near–real-time monitoring.
Meaning Results from near–real-time monitoring of health outcomes after BNT162b2 COVID-19 vaccination are consistent with current evidence and provide additional evidence of vaccine safety in the pediatric population.
An epidemiologist asks the right questions.
JAMA Peds publishes myo/peri study on kids - without stratifying for male/female? And threw out 75% of cases due to not having medical records to review?
She then also asks: “The rates appear to be based on 37 of 153 cases. Would there be signals for other events if cases were not discarded due to lack of medical records for review? Do we distrust the codes in these active surveillance databases that much? Or is this convenient to reduce the signal?”
Here’s some text from the study:
“Of the 153 cases of myocarditis or pericarditis among children aged 12 to 17 years, medical record review was conducted for a sample of 37 cases whose records were obtainable. Twenty-seven of these cases (73.0%) were confirmed as true cases of myocarditis or pericarditis, of which 25 patients were male, and 19 were hospitalized with a mean length of hospital stay of 2.8 days (median, 2 days). The mean time from vaccination to presentation for care for myocarditis or pericarditis was 6.8 days (median, 3 days).”
92% of confirmed cases were males. So she’s quite right. Where are the gender-stratified results?
The authors also wrote:
“We did not detect a signal for myocarditis or pericarditis in younger children (aged 5-11 years), which is consistent with reports from other surveillance systems.”
Close inspection shows that one of the high relative risk values, which for one database for one age group was a record-breaking RR = 50.01, was in fact elevated in 5-11 year-old vaccinees.
{kind=link}
RR = 3.49 and 10.29???
They did not find these results?
Dropping the 75% without medical records no doubt reduced the statistical power, the same trick used by the infamous Destefano et al study (2004) to make the association between on-time MMR vaccines and autism go away after rigorous p-hacking.
...
Myocarditis: Once Rare, Now Common | A Comprehensive Review of Myocarditis, Covid and COVID vaccines
As an actively practicing clinical cardiologist for many years in three different communities, I knew about myocarditis. I just never saw it. Quite literally, I recall seeing ONE young woman who presented with a picture of acute congestive heart failure, and her echocardiogram study revealed a big and poorly contracting heart. Such a condition is diagnosed as an idiopathic congestive cardiomyopathy, which basically means the heart is enlarged and functioning very poorly, and you have no idea why. After treating her with traditional measures for congestive heart failure, she started getting better. To my great surprise, after six to nine months of follow-up, her echocardiogram had returned to normal. ...
COVID and Myocarditis
Today, the active clinical cardiologist is seeing myocarditis patients on a regular basis. The scientific literature indicates that myocarditis is occurring quite frequently in patients harboring the chronic presence of the COVID-related spike protein. This is being seen in many individuals with persistent chronic COVID, many of whom have been vaccinated, as well as in a substantial number of individuals who have been vaccinated and have never contracted COVID. A study in mice showed that the injection of the mRNA vaccine (which produces the spike protein) reliably induced myopericarditis. Regardless of the initial source of exposure to spike protein, it appears to be the reason for the pathology and symptoms seen in chronic COVID.
While not yet clearly documented by any well-designed studies in the medical literature, a great deal of anecdotal information indicates that vaccine mRNA shedding can occur. And once transmitted, the mRNA directly leads to spike protein production. Such mRNA shedding means that the spike protein is indirectly, if not directly as well, transmissible from one individual to another via inhalation or various forms of skin contact.
In fact, Pfizer's own internal documents advise about the possibility of "environmental exposure" by "inhalation or skin contact" of the mRNA in the vaccine being transmitted from a vaccinated individual to another person. Furthermore, while many try to dismiss such an "exposure" as too minimal to be of clinical consequence, such an assertion cannot be assumed to be true when dealing with an agent (spike protein) that appears capable of replication once it gains access to the body. The toxicity associated with spike protein would not be due to a one-time exposure, but one that could persist indefinitely because of this ability to replicate. A toxin that has such an ability is truly a clinical nightmare. It is never a good idea to overestimate the integrity of the pharmaceutical industry.
much, much more ...
...
First our quick one-liner summaries for your tweeting pleasure: FDA finally admits in its own report on 65+ mRNS recipients: Risk of lung clots up 50% - Risk of heart attacks up 40%+ https://www.sciencedirect.com/science/article/pii/S0264410X22014931
Jan 2022, JAMA study found myocarditis risk increased in multiple age, sex groups after mRNA COVID-19 vaccination, highest in young men. https://jamanetwork.com/journals/jama/fullarticle/2788346
Study of VAERS data between Jan-Jun 2021 found highest rate of myocarditis in young boys 12-15 after dose 2 of mRNA COVID-19 vaccination. https://onlinelibrary.wiley.com/doi/10.1111/eci.13759
This slide presentation to the CDC and FDA on myocarditis should have rung some IMMEDIATE alarms bells - but we went on vaxxing the young lads anyway. https://fda.gov/media/159007/download
Study in Nature found increased risks of myocarditis and pericarditis in France after Covid-19 mRNA vaccines, particularly after 2nd dose and in age 18-24 yrs, both male and female were affected. https://www.nature.com/articles/s41467-022-31401-5
CDC report 2022 found 14 cases of myocarditis or pericarditis among 102,091 males aged 16-17 who received Pfizer-BioNTech Covid-19 vaccine, significant departure from reported rates in 2021, showing concerns labeled as misinformation are real. https://thefederalist.com/2022/09/09/cdc-admits-post-vaccine-myocarditis-concerns-that-were-labeled-covid-misinformation-are-legit/
Study found myocarditis/pericarditis as rare side effect of mRNA COVID-19 vaccines, disproportionately affects young male adolescents, commonly after 2nd dose of primary series and 1st booster. https://www.acpjournals.org/doi/10.7326/M22-2274
The estimated MMRRs and SMR were about 4 times higher than the MMRRs and SMR. The study concludes that the SARS-CoV-2 vaccine is associated with a higher risk of myocarditis death in all age groups, including the elderly. The risk may be 4 times or higher than the apparent risk of myocarditis death. https://www.medrxiv.org/content/10.1101/2022.10.13.22281036v1.full.pdf
Markedly elevated levels of full-length spike protein were detected in the plasma of individuals with post-vaccine myocarditis, whereas no free spike was detected in asymptomatic vaccinated control subjects. It suggests that the cause of myocarditis may be linked with spike antigen. https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.122.061025
The risk ratio for the mRNA vaccines combined is 1.43 which means that recipients are 43% more likely to have a serious adverse event. https://www.sciencedirect.com/science/article/pii/S0264410X22010283
You’re going to have to vax 35K young adults to prevent one hospitalization and in doing so you’re going to send nearly 20 of these folks into a serious adverse reaction from the vax. https://jme.bmj.com/content/early/2022/12/05/jme-2022-108449
...
Of the few studies that even attempt to assess the population-wide risk of myocarditis following vaccination, nearly three-fourths neglect to include the proper stratifiers
...
…
This article seems to suggest that autopsies are the only main way to test vaccine injuries for sure, as it explored the strong possibility of long term effects of the vaccine.
Reuters is trying to say that hospitalizations didn't skyrocket in 2021, they are trying to say that data was so poorly reported between 2016-2021 that a 300 percent increase, in some cases, is now just back to normal, and there are no problems with reporting currently, of course.
Risk of Myocarditis After Sequential Doses of COVID-19 Vaccine and SARS-CoV-2 Infection by Age and Sex
‘Spikeopathy’: COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA
First-hand information from senior nurses who work in emergency rooms, hospital wards and intensive care units regarding unprecedented amounts of young people presenting with cancers, strokes, and heart attacks.
Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial.
Systematic Review of Autopsy Findings in Deaths after COVID-19 Vaccination (Independent study)
Pfizer and Moderna dodge questions and plead ignorance at Senate hearing
Florida Health Alert (with some relevant links to data on COVID vaccine injury)
Jeffrey Sachs, Ph.D., chair of the COVID-19 Commission for the Lancet, one of the most prestigious and oldest peer-reviewed general medical journals, presents evidence of possible lab origin of Covid-19
"Surgisphere", A fake company, were able to get wildly incorrect studies about the "dangers" of a known remedy for COVID published in Lancet, a well-regarded scientific journal.
DNA contamination in mRNA vaccines
Florida calls the COVID vaccine a "bioweapon" and seeks to make it illegal
“Nevertheless, the expert group believes that, for some of these frail patients, common adverse reactions may have contributed to a more serious course of their disease.”
Are Covid Vaccines Riskier Than Advertised?
in the FDA who refuse to take the jab
Censored Scientific Journal from 2021 detailing deaths caused by the vaccine.
Another Scientific Journal Linking Myocarditis to the COVID Vaccines
47-year-old UK man faces speech issues and memory reduction after Covid vaccine, seeks compensation for brain injury
The British Medical Journal has investigated the CDC's vaccine surveillance efforts and deems the system "overwhelmed."
"Dr. Gatti’s 2017 study showed an incredible amount of contamination in a whole host of traditional vaccines in the form of tiny nanoparticles, mostly metallic."
Ignored Danger Signals: Newly Released Pfizer Trial Data Shows 8 Sudden Deaths in Vaccinated Subjects Vs. Just 4 Sudden Deaths in the Unvaccinated
31% of women who were exposed to COVID-19 products prior to pregnancy experienced a miscarriage according to VAERS domestic data
Another compendium of a compendium:
What is the link between Covid Vaccines and strokes in the medicinal literature?
Cerebral venous sinus thrombosis in the U.S. population after SARS-CoV-2 vaccination with adenovirus and after COVID-19:
Cerebral venous sinus thrombosis negative for anti-PF4 antibody without thrombocytopenia after immunization with COVID-19 vaccine in a non-comorbid elderly Indian male treated with conventional heparin-warfarin based anticoagulation.
Cerebral venous thrombosis after BNT162b2 mRNA SARS-CoV-2 vaccine.
Cerebral venous sinus thrombosis after vaccination: the United Kingdom experience.
US case reports of cerebral venous sinus thrombosis with thrombocytopenia after vaccination with Ad26.COV2.S (against covid-19), March 2 to April 21, 2020.
Management of cerebral and splanchnic vein thrombosis associated with thrombocytopenia in subjects previously vaccinated with Vaxzevria (AstraZeneca): position statement of the Italian Society for the Study of Hemostasis and Thrombosis (SISET).
Vaccine-induced immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis after vaccination with COVID-19; a systematic review.
Early results of bivalirudin treatment for thrombotic thrombocytopenia and cerebral venous sinus thrombosis after vaccination with Ad26.COV2.S.
A rare case of a middle-aged Asian male with cerebral venous thrombosis after AstraZeneca COVID-19 vaccination.
Cerebral venous sinus thrombosis and thrombocytopenia after COVID-19 vaccination: report of two cases in the United Kingdom.
Diagnostic-therapeutic recommendations of the ad-hoc FACME expert working group on the management of cerebral venous thrombosis related to COVID-19 vaccination.
COVID-19 vaccination: information on the occurrence of arterial and venous thrombosis using data from VigiBase.
Cerebral venous thrombosis associated with the covid-19 vaccine in Germany.
Cerebral venous thrombosis following BNT162b2 mRNA vaccination of BNT162b2 against SARS-CoV-2: a black swan event.
The importance of recognizing cerebral venous thrombosis following anti-COVID-19 vaccination.
Cerebral venous sinus thrombosis negative for anti-PF4 antibody without thrombocytopenia after immunization with COVID-19 vaccine in an elderly, non-comorbid Indian male treated with conventional heparin-warfarin-based anticoagulation.
Vaccine-induced immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis after covid-19 vaccination; a systematic review.
A rare case of cerebral venous thrombosis and disseminated intravascular coagulation temporally associated with administration of COVID-19 vaccine.
Acute cerebral venous thrombosis and pulmonary artery embolism associated with the COVID-19 vaccine.
Cerebral venous thrombosis and vaccine-induced thrombocytopenia.a. Oxford-AstraZeneca COVID-19: a missed opportunity for a rapid return on experience.
Diagnosis and treatment of cerebral venous sinus thrombosis with vaccine-induced immune-immune thrombotic thrombocytopenia.
Venous sinus thrombosis after vaccination with ChAdOx1 nCov-19:
Cerebral venous sinus thrombosis following vaccination against SARS-CoV-2: an analysis of cases reported to the European Medicines Agency.
Arterial events, venous thromboembolism, thrombocytopenia and bleeding after vaccination with Oxford-AstraZeneca ChAdOx1-S in Denmark and Norway: population-based cohort study.
Cerebral venous thrombosis associated with COVID-19 vaccine in Germany:
Malignant cerebral infarction after vaccination with ChAdOx1 nCov-19: a catastrophic variant of vaccine-induced immune-mediated thrombotic thrombocytopenia.
Cerebral venous sinus thrombosis associated with thrombocytopenia after COVID-19 vaccination.
Central venous sinus thrombosis with subarachnoid hemorrhage after COVID-19 mRNA vaccination: are these reports merely coincidental:
Cerebral venous sinus thrombosis negative for anti-PF4 antibody without thrombocytopenia after immunization with COVID-19 vaccine in a non-comorbid elderly Indian male treated with conventional heparin-warfarin-based anticoagulation.
Cerebral venous sinus thrombosis 2 weeks after first dose of SARS-CoV-2 mRNA vaccine.
Deep venous thrombosis (DVT) occurring shortly after second dose of SARS-CoV-2 mRNA vaccine.
Vaccine-induced immune thrombotic thrombocytopenia causing a severe form of cerebral venous thrombosis with high mortality rate: a case series.
Procoagulant microparticles: a possible link between vaccine-induced immune thrombocytopenia (VITT) and cerebral sinus venous thrombosis.
Acute cerebral venous thrombosis and pulmonary artery embolism associated with the COVID-19 vaccine.
Cerebral venous thrombosis following COVID-19 vaccination.
Adverse effects reported after COVID-19 vaccination in a tertiary care hospital, centered on cerebral venous sinus thrombosis (CVST)
Cerebral venous thrombosis associated with COVID-19 vaccine in Germany:
Cerebral venous sinus thrombosis after COVID-19 vaccination : Neurological and radiological management.
Cerebral venous thrombosis and thrombocytopenia after COVID-19 vaccination.
Cerebral venous sinus thrombosis and thrombocytopenia after COVID-19 vaccination: report of two cases in the United Kingdom.
Cerebral venous thrombosis induced by SARS-CoV-2 vaccine.
Cerebral venous sinus thrombosis associated with vaccine-induced thrombotic thrombocytopenia.
Cerebral venous thrombosis after the BNT162b2 mRNA SARS-CoV-2 vaccine.
Cerebral venous thrombosis after COVID-19 vaccination.
Lethal cerebral venous sinus thrombosis after COVID-19 vaccination:
Cerebral venous sinus thrombosis in the U.S. population, After SARS-CoV-2 vaccination with adenovirus and after COVID-19.
Cerebral venous thrombosis after COVID-19 vaccination: is the risk of thrombosis increased by intravascular administration of the vaccine?
Central venous sinus thrombosis with subarachnoid hemorrhage after COVID-19 mRNA vaccination: are these reports merely coincidental
Cerebral venous sinus thrombosis after ChAdOx1 nCov-19 vaccination with a misleading first brain MRI
Early results of bivalirudin treatment for thrombotic thrombocytopenia and cerebral venous sinus thrombosis after vaccination with Ad26.COV2.S
…
The real Covid jab scandal is finally emerging | The young and healthy, who were at minimal risk from Covid, should not have been told they had to take the vaccine.
Texas Gov. Greg Abbott signs bill banning COVID-19 vaccine mandates by private employers.
Cambridge professor cautious about calling vaccines ‘safe and effective’
Families of AstraZeneca vaccine victims fight to get jab listed on death certificates
145-Country Study Shows Increase Of Transmission And Death After Introduction Of Covid Vaccines
Infant mortality rates regressed against number of vaccine doses routinely given: Is there a biochemical or synergistic toxicity?
Swiss Policy Research: DNA Contamination in Pfizer and Moderna Covid Vaccines | "The potential pharmaceutical and clinical effects of the newly discovered plasmid DNA fragments in Pfizer and Moderna covid vaccines need to be investigated very carefully."
The Telegraph: Oxford AstraZeneca Covid jab was ‘defective’, claims landmark legal case }| Victims of VITT - a new condition identified by specialists - question the Government's monitoring of the vaccine's rollout and its efficacy.
Sex-specific differences in myocardial injury incidence after COVID-19 mRNA-1273 booster vaccination | "Among 777 participants, 40 participants (5.1%) had elevated hs-cTnT concentration on day 3 and mRNA-1273 vaccine-associated myocardial injury was adjudicated in 22 participants (2.8%)."
Cardiac side effects of RNA-based SARS-CoV-2 vaccines | "Our present data suggest that the risk–benefit ratio of mRNA-based vaccines should be re-evaluated taking into consideration of current preclinical cardiac safety data"
Australian Government's Health Authorities Baffled by Excess Deaths. | “I witnessed the first vaccine induced deaths within a week of the commencement of their use. As a clinician, it doesn't take armies of statisticians for me to be cognisant of a deadly drug.”
Israeli MoH data proves the vaccines are killing people. How come nobody noticed? | In March 2023, MIT Professor Retsef Levi disclosed a troubling figure produced by the Israeli Ministry of Health. This is unassailable proof the vaccines are killing people.
Excess mortality in the 20 most vaccinated highly developed countries almost triples! Median all-cause excess mortality in the 20 most vaccinated highly developed countries increased by +149% after vaccination rollout!
Questioning Lipid Nanoparticles | mRNA shots differ completely from all other previously available “vaccine” products, not only because of their mRNA component, but also because of LNP components.
Study Data Showed Vaccinated Kids Shed COVID Up to 3 Times Longer Than Unvaxed — But Authors Concluded They Were ‘Equally Contagious’
Oxford AstraZeneca Covid jab was ‘defective’, claims landmark legal case.
MSM reporting several instances where COVID-19 vaccine deaths were not reported as such until relatives fought to set the record straight. New study also shows twice the number of sudden deaths in Pfizer's trial amongst the vaccinated. Also the case of the 'unjabbed COVID death' subject who actually died days after taking the Moderna jab.
Newer COVID-19 vaccines: Still lights and shadows? | "Thus, an enhanced malfunction of ACE2 receptors is not to be excluded. In other words, new COVID-19 vaccines (2023–2024) might be associated with an increased risk of adverse reactions when compared with previous formulations."
Preprint: "Among those with previous SARS-CoV-2 infection(s), when comparing two vs. three Wuhan vaccine doses, there was no observed difference between groups. Additional Wuhan platform mRNA vaccines did not improve NtAb response to BA.4/5, but prior SARS-CoV-2 infection enhances NtAb response."
LONG-TERM COVID-19 BOOSTER EFFECTIVENESS AND IMMUNE IMPRINTING | "Effectiveness was highest at 57.1% in the 1st month after the booster but waned and was modest at only 14.4% by the 6th month. In the 7th month and thereafter, effectiveness was progressively negative reaching -20.3% after one year."
Nature: Duration of SARS-CoV-2 mRNA vaccine persistence and factors associated with cardiac involvement in recently vaccinated patients | "These results suggest that SARS-CoV-2 mRNA vaccines routinely persist up to 30 days from vaccination and can be detected in the heart."
Circulation: Circulating Spike Protein Detected in Post–COVID-19 mRNA Vaccine Myocarditis | "Markedly elevated levels of full-length spike protein were detected in the plasma of individuals with postvaccine myocarditis, whereas no free spike was detected in asymptomatic vaccinated control subjects."
Rapid Progression of Angioimmunoblastic T Cell Lymphoma Following BNT162b2 mRNA Vaccine Booster Shot: A Case Report
Mortality increases dramatically after the shot. This is true for all doses, in all 5 countries we have data on. See Medicare death data confirms the COVID vaccines are killing people. No more doubts. Same anomaly in all 5 countries.
Federal Judge Orders CDC to Release All V-safe Free-Text Entries in a Huge Win for Vaccine Safety Transparency
New research finds the natural seasonality of coronaviruses had more influence on the COVID-19 pandemic than government interventions including vaccinations, lockdowns, masks and travel restrictions
What Covid vaccine manufacturers did not check - Safety of synthetic mRNA 'far from completely understood'
"Conclusion: When compared with nonvaccinated patients, asymptomatic patients who received their second vaccination 1–180 days prior to imaging showed increased myocardial 18F-FDG uptake on PET/CT scans."
This study compared the self-reported incidence of Long COVID in twice vaccinated, once vaccinated, or unvaccinated. Using unvaccinated as the reference, the once vaccinated were 1.88 times more likely to report Long COVID symptoms 6 months later and the twice vaccinated were 2.32 times more likely to report Long COVID symptoms 6 months later. See Table 4.
Two Sudden Cardiac Vaccinated Deaths in Pfizer’s COVID Vaccine Clinical Trial Not Disclosed to FDA with EUA Data | "If the deaths had been disclosed in the EUA submission, they would have shown that the BNT162b2 mRNA COVID vaccine intervention did not reduce deaths."
Long term follow up and outcomes of Covid-19 vaccine associated myocarditis in Victoria, Australia | "There appears to be a significant proportion of patients (54.8%) who experience ongoing symptoms 6 months post onset."
Study Finds COVID Vaccination Independently Associated With Long COVID Syndrome
"COVID-19 vaccination-related glomerular (kidney) diseases have become a new concern. Both the mRNA vaccine and the inactivated vaccine can cause new-onset and relapsing glomerular (kidney) disease. These diseases typically occur after the first or second dose of vaccination."
Series of studies from South Korea raise serious concerns | Yet more signals of systemic vaccine harms
“Do People Care Enough About Each Other to Speak Out Against Catastrophic 'Vaccines'? It's past the time to continue to tolerate this "mRNA vaccine experiment.” We were promised that the COVID-19 shots were going stop the spread of the ‘virus’ and end the pandemic. We were lied to.”